A lot of people are very angry with Martin Shkreli. Shkreli is CEO of Turing Pharmaceuticals. Turing recently purchased the rights to Daraprim, a drug that treats toxoplasmosis, a condition that poses the greatest threat to people with weakened immune systems, such as AIDS patients. 4,400 people are hospitalized with the condition each year in the US, and about 327 people die on average each year. Once Turing acquired Daraprim, it promptly raised the price from $13.50 per pill to $750. Turing and Shkreli claimed that the price increase was necessary to make a profit and to pay for research and development into new toxoplasmosis drugs, but the medical establishment and the public strongly disagree. Dr. David Relman, chief of infectious diseases at VA Palo Alto Healthcare System, told Fortune:
We are not in dire need of new drugs for toxoplasmosis right now. There is no significant drug resistance problem with toxoplasmosis. We do not need them to be undertaking some self-serving marketing campaign. There is no public health need for such. This is simply about greed.
The HIV Medicine Association and the Infectious Diseases Society of America concurred, writing a joint letter condemning the move. But in going after Shkreli and Turing individually, we’re collectively missing the point–they are a symptom of a much larger prescription drug problem in America.

Why did Shkreli raise the price in the first place? Because in the United States, we have created an incentive structure that undeniably makes this the smart thing for him to do. We have a privatized healthcare system, and this means that drug companies operate under the profit motive–they produce whatever drugs it is most profitable to produce and sell them at whatever price yields the greatest possible profit. It makes no different whatsoever to them whether it might save more lives or relieve more suffering to produce different drugs or sell them at a lower cost. Our system does not give them any reasons whatsoever to care about suffering or human lives. People respond to the incentive structures our government creates. When they behave appallingly, we should not blame them, we should blame our government–it has not merely allowed them to do what they’re doing, it has actively incentivized it by perpetuating a healthcare system in which immense profits can be made from this behavior.
Defenders of current policies argue that by allowing these companies to make large profits we increase the amount of money they are able to invest more in research and development. This argument may be a bit over-hyped. While it’s true that in raw terms, US pharmaceutical companies spend far more on R&D (49% of the global total), the difference is negligible on a per capita basis. British pharmaceutical companies account for 9% of the global total in R&D spending, but the US population is about 5 times bigger than Britain’s. If Britain were as large as the US, its pharmaceutical companies might account for 45% to America’s 49%–a mere 4 points of difference. This is important, because Britain’s prescription drug costs are not merely a little bit lower than America’s, they’re drastically lower. Here are international comparisons for three major drugs–Nexium, Plavix, and Lipitor:



Ignore the Medicare figures–they’re outdated. In each case, the lowest US private insurance cost the researchers could find was more than twice as high as the UK cost, and for Nexium and Lipitor the US low was more than three times as high. The highest US figure they found was in all three cases astronomical. Neighboring Canada was much cheaper too, but despite this federal law does not currently allow imported Canadian or other international pharmaceuticals to compete with domestically produced pills. This unnecessarily mercantilist policy prevents American drug companies from facing any kind of competition, creating false scarcity and inflating prices. Most of the money raised by pharmaceutical companies does not even go to research and development and instead funds marketing:

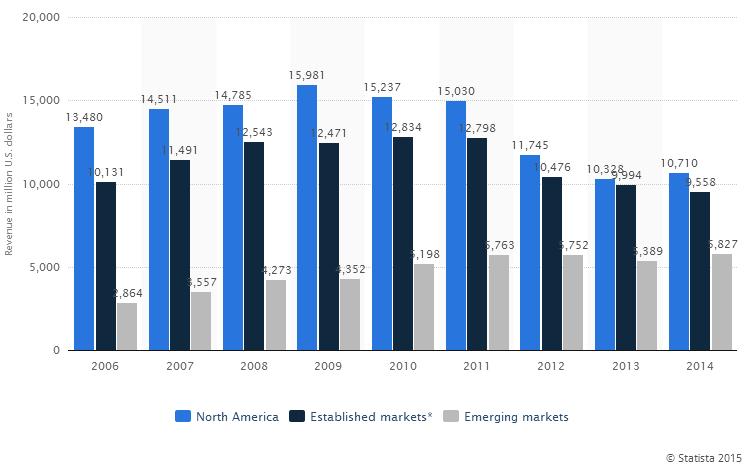
But suppose this is all wrong–suppose that these high prices do allow a lot of R&D that would not otherwise take place. Many British pharmaceutical companies market drugs in the United States–it’s always possible that US sales provide the bulk of their profits. In the case of British multinational AstraZeneca, the North American market (the US, but also Canada) does provide the largest portion of sales, but not half of the total:
If it is true that even foreign drug companies rely on the US for R&D funding, this still would not justify the current scheme of high US drug prices for two reasons:
- It’s unnecessarily regressive–it forces poor and middle income Americans to pay the cost of financing R&D when this cost could instead be distributed in a more progressive, egalitarian way.
- This would mean that we are forcing American patients to disproportionately subsidize R&D for the rest of the world, because American patients pay far more for the same medications than the people of any other major country.
There are many better ways to manage our pharmaceuticals. The most exciting, effective and radical strategy I can think of would involve nationalizing the pharmaceutical industry outright. The government could then provide drugs at cost, sharply reducing prices. We could then levy a progressive tax to pay for R&D. This tax could raise far less money than we currently pay in prescription drug costs, because the government would not need to spend any money at all on marketing or sales. What’s more, the R&D we would conduct would be motivated not by a desire to generate profit, but by a desire to improve patient outcomes. This means that the research we would conduct would be better targeted to meet patient needs.
Unfortunately, “nationalization” remains a dirty word in the United States, and there are many people who will not consider nationalization even in cases where it makes a great deal of sense economically and would make an industry far more efficient and effective. So what else can we do? We could switch to a single payer system based on Medicare-for-all. Bernie Sanders wants to do this. Single payer would give us a healthcare system far more similar to the UK’s or Canada’s. With single payer, there is one insurance company–the government–and it negotiates prices with pharmaceutical companies on behalf of the entire population. This means that the government can effectively fix its own prices for drugs and medical care. It has to set prices high enough to ensure that enough people will become doctors and that pharmaceutical companies can stay in business, but outside of that it is able to drive a very hard bargain. This would give us prescription drug costs that are similar to the UK’s or Canada’s. What it cannot do is force the prescription drug companies to spend what they are given on R&D, much less ensure that the R&D the drug companies do finance is the R&D we really need. This is why even with a single payer system, we would be best off nationalizing the pharmaceutical industry. The two policies in combination would both drive down our costs and enable us to better target our R&D funds.
But like nationalization, “single payer” is also a dirty word in the United States. So what else can we do? Bernie Sanders recognizes that it is highly unlikely that he would be able to get single payer passed if he were elected president, so he has additionally proposed a more modest reform package. He’s introduced a bill in the senate that would do a number of different things:
- It allows Medicare to better use its leverage to negotiate drug prices collectively for its entire patient pool.
- It allows the importation of prescription drugs from Canada, to increase competition.
- It requires drug companies to pay rebates to low income patients.
- It prevents brand-name drugs from paying to keep generic versions of their drugs off the market.
- It strips drug companies of government-backed monopolies if they are found guilty of fraud.
- It forces drug companies to make a public report on the amount they are spending on R&D, marketing, and so on.
This legislation would make a significant dent in the problem, though I doubt it will be passed–pharmaceutical companies spend almost $240 million per year on lobbying in the United States:
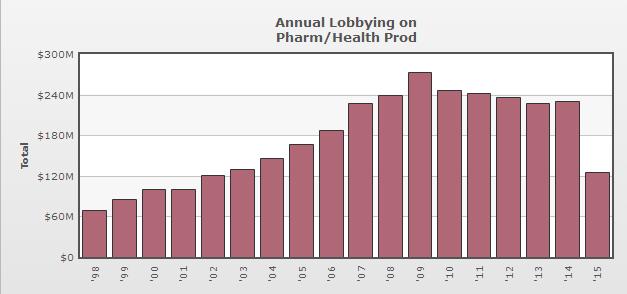
This is far more than any other industry in the country–almost $90 million more than the oil and gas companies spend, and about 133 times more than the NRA spends fighting gun control laws. When you’re getting a deal as good as big pharma is in this country, a couple hundred million to defend your turf is trivial.
Should we expect anything less? Our political system enables and encourages wealthy industries to spend comparatively small percentages of their profits effectively bribing politicians to ignore the damage our current policies and incentive structures are doing. Our political system itself is an incentive structure that incentivizes perpetuating perverse incentive structures. Martin Shkreli is a prick, but he’s our product. Until we make the necessary policy and structural changes, he’s just another prick in our nation’s perpetual prick parade.
